
The race is on to find a vaccine against the new COVID-19 coronavirus. Professor Jonathan Heeney explains why a cautious approach is needed and how his team is using new technology developed for influenza and Ebola viruses to target the new infection.
It is hard now to conceive that two months ago, few people had heard of the new coronavirus. Now, the virus, which causes the disease COVID-19, has spread to every corner of the globe. The World Health Organization has officially declared the outbreak a pandemic.
With the threat of hundreds of thousands – possibly millions – of people being infected and healthcare systems becoming overwhelmed, the race is on to develop a vaccine that will protect individuals and slow the spread of the disease. But Professor Jonathan Heeney, Head of the Laboratory of Viral Zoonotics at the University of Cambridge, and one of the people working on a vaccine, says that coronaviruses present a particular challenge to vaccine developers.
Coronaviruses are named after their appearance: they are spherical objects, on the surface of which sit ‘spike’ proteins. The virus uses these spikes to attach to and invade cells in our body. Once inside, the virus uses the cell’s own machinery to help itself replicate and spread throughout the body, causing disease and allowing it to transmit onwards.
Traditionally, scientists would develop vaccines that programme the body to produce antibodies that recognise and block these spikes. But this strategy can misfire with coronaviruses due to a phenomenon known as ‘antibody-induced enhancement’ or ‘vaccine-induced enhancement’, says Heeney.
“If you make antibodies against the spike, they can end up binding to it and helping the virus invade important immune cells known as monocyte-macrophages. Rather than destroying the virus, these cells can then end up being reprogrammed by the viruses, exacerbating the immune response and making the disease much, much worse than it would otherwise be.”


 “Life begins at 55, the age at which I published my first book,” he wrote in “From Eros to Gaia,” one of the collections of his writings that appeared while he was a professor of physics at the Institute for Advanced Study — an august position for someone who finished school without a Ph.D. The lack of a doctorate was a badge of honor, he said. With his slew of honorary degrees and a fellowship in the Royal Society, people called him Dr. Dyson anyway.
“Life begins at 55, the age at which I published my first book,” he wrote in “From Eros to Gaia,” one of the collections of his writings that appeared while he was a professor of physics at the Institute for Advanced Study — an august position for someone who finished school without a Ph.D. The lack of a doctorate was a badge of honor, he said. With his slew of honorary degrees and a fellowship in the Royal Society, people called him Dr. Dyson anyway.
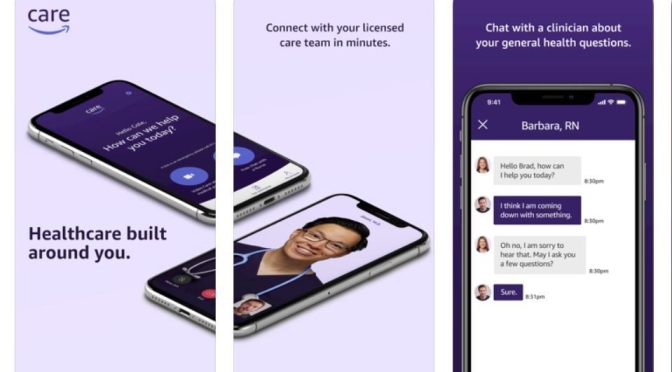
 Amazon’s virtual medical clinic that offers in-person follow-ups is now available to Amazon employees in Seattle.
Amazon’s virtual medical clinic that offers in-person follow-ups is now available to Amazon employees in Seattle. 3. Medications prescribed via Amazon Care can be delivered to a patient’s home.
3. Medications prescribed via Amazon Care can be delivered to a patient’s home.
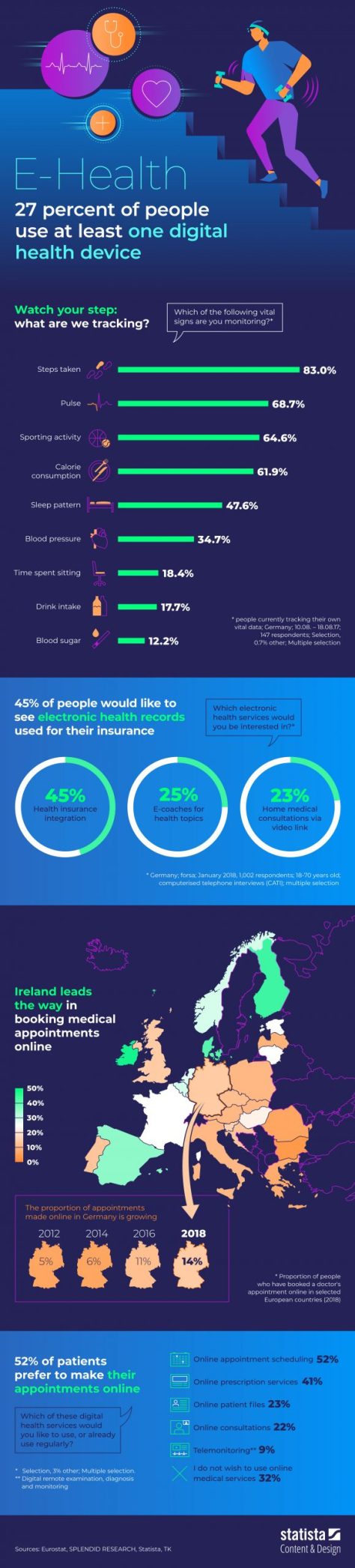
 Many Americans are willing to make significant personal tradeoffs to lower their health insurance rates or medical costs, such as agreeing to 24/7 personal monitoring or working with artificial intelligence instead of a human doctor, the Center for the Digital Future at the USC Annenberg School for Communication and Journalism finds.
Many Americans are willing to make significant personal tradeoffs to lower their health insurance rates or medical costs, such as agreeing to 24/7 personal monitoring or working with artificial intelligence instead of a human doctor, the Center for the Digital Future at the USC Annenberg School for Communication and Journalism finds.


