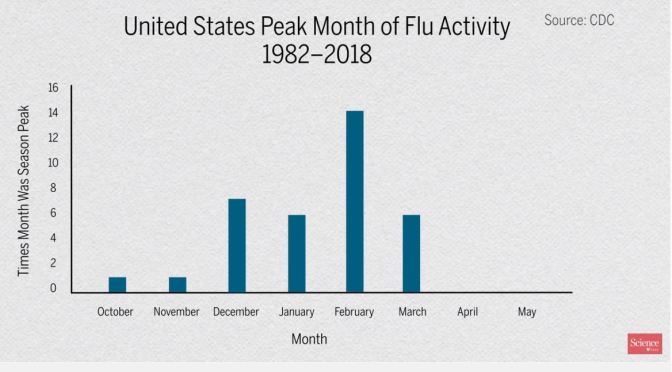
On this week’s show, host Joel Goldberg gets an update on the coronavirus pandemic from Senior Correspondent Jon Cohen. In addition, Cohen gives a rundown of his latest feature, which highlights the relationship between diseases and changing seasons—and how this relationship relates to a potential coronavirus vaccine.
Also this week, from a recording made at this year’s AAAS annual meeting in Seattle, host Meagan Cantwell speaks with Alexandra Maertens, director of the Green Toxicology initiative at Johns Hopkins University, Baltimore, about the importance of incorporating nonanimal testing methods to study the adverse effects of chemicals.
Scientists and doctors have observed for thousands of years that some diseases, like polio and influenza, rise and fall with the seasons. But why? Ongoing research in animals and humans suggests a variety of causes, including changes in the environment (like pH, temperature, and humidity) and even seasonal and daily changes to our own immune systems. Figuring out those answers could one day make all the difference in minimizing the impact of infectious disease outbreaks—such as COVID-19.
Though U.S. legislation targeting the problem of surprise medical bills advanced out of key congressional committees in 2019 with support from leaders in both parties, Congress ultimately failed to pass a law to end such bills.
Erin Fuse Brown is an associate professor of law at Georgia State University. Stephen Morrissey, the interviewer, is the Executive Managing Editor of the Journal.
On the Mayo Clinic Q&A podcast, Dr. Jessica Lancaster, a Mayo Clinic immunologist, discusses aging and the immune system. Some people are at higher risk of getting very sick from COVID-19 because of their age or underlying health conditions, according to the Centers for Disease Control and Prevention (CDC).
Adults 60 and older and those with an underlying health condition or a compromised immune system appear to develop serious illness more often than others. This interview was recorded March 19, 2020.
Chloroquine was shown in 2004 to be active in vitro against SARS coronavirus but is of unproven efficacy and safety in patients infected with SARS-CoV-2. The drug’s potential benefits and risks for COVID-19 patients, without and with azithromycin, is discussed by Dr. David Juurlink, head of the Division of Clinical Pharmacology and Toxicology at Sunnybrook Health Sciences Centre in Toronto.
From Wall Street Journal article:
Our experience suggests that hydroxychloroquine, with or without a Z-Pak, should be a first-line treatment. Unfortunately, there is already a shortage of hydroxychloroquine. The federal government should immediately contract with generic manufacturers to ramp up production. Any stockpiles should be released.
As a matter of clinical practice, hydroxychloroquine should be given early to patients who test positive, and perhaps if Covid-19 is presumed—in the case of ill household contacts, for instance. It may be especially useful to treat mild cases and young patients, which would significantly decrease viral transmission and, as they say, “flatten the curve.”
As many businesses around the world struggle, a Canadian disinfectant company is increasing production to keep up with demand during the novel coronavirus outbreak. Photo: Ron Kolumbus/WSJ
The race is on to find a vaccine against the new COVID-19 coronavirus. Professor Jonathan Heeney explains why a cautious approach is needed and how his team is using new technology developed for influenza and Ebola viruses to target the new infection.
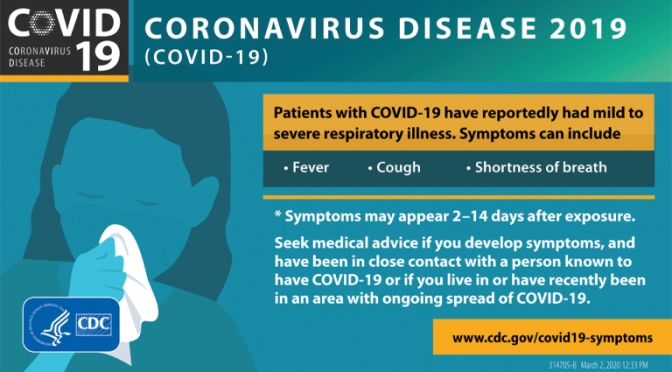
It is hard now to conceive that two months ago, few people had heard of the new coronavirus. Now, the virus, which causes the disease COVID-19, has spread to every corner of the globe. The World Health Organization has officially declared the outbreak a pandemic.
With the threat of hundreds of thousands – possibly millions – of people being infected and healthcare systems becoming overwhelmed, the race is on to develop a vaccine that will protect individuals and slow the spread of the disease. But Professor Jonathan Heeney, Head of the Laboratory of Viral Zoonotics at the University of Cambridge, and one of the people working on a vaccine, says that coronaviruses present a particular challenge to vaccine developers.
Coronaviruses are named after their appearance: they are spherical objects, on the surface of which sit ‘spike’ proteins. The virus uses these spikes to attach to and invade cells in our body. Once inside, the virus uses the cell’s own machinery to help itself replicate and spread throughout the body, causing disease and allowing it to transmit onwards.
Traditionally, scientists would develop vaccines that programme the body to produce antibodies that recognise and block these spikes. But this strategy can misfire with coronaviruses due to a phenomenon known as ‘antibody-induced enhancement’ or ‘vaccine-induced enhancement’, says Heeney.
“If you make antibodies against the spike, they can end up binding to it and helping the virus invade important immune cells known as monocyte-macrophages. Rather than destroying the virus, these cells can then end up being reprogrammed by the viruses, exacerbating the immune response and making the disease much, much worse than it would otherwise be.”
\This video from Harvard Medical School’s HMX Fundamentals Immunology online course offers a high-level overview of the immune system at work in the context of daily life.
In order to stem the spread of the coronavirus, social interactions around the world are being restricted. This infographic, based on calculations by Robert A. J. Signer, Assistant Professor of Medicine at the University of California San Diego, shows how this so-called social distancing can reduce the spread of the virus.
With no changes to social behaviour, one infected person will on average pass the virus to 2.5 people within five days. After 30 days, the figure would rise to a devastating 406 new infections. The number can be significantly reduced though by engaging in less social contact. With a 50 percent reduction, the number of new infections caused by the average person after 30 days is just 15 people. A 75 percent change would result in an even lower 2.5 new cases – greatly reducing the burden on health services and, if followed by everybody, allowing a country to ‘flatten the curve’ of new infections.
News, Views and Reviews For The Intellectually Curious


 On this week’s show, host Joel Goldberg gets an update on the coronavirus pandemic from Senior Correspondent Jon Cohen. In addition, Cohen gives a rundown of his latest feature, which highlights the relationship between diseases and changing seasons—and how this relationship relates to a potential coronavirus vaccine.
On this week’s show, host Joel Goldberg gets an update on the coronavirus pandemic from Senior Correspondent Jon Cohen. In addition, Cohen gives a rundown of his latest feature, which highlights the relationship between diseases and changing seasons—and how this relationship relates to a potential coronavirus vaccine.