For the past 10 to 15 years, virtual health has been heralded as the next disrupter in the delivery of care, but there has been minimal uptick in adoption. The COVID-19 pandemic is pushing against structural barriers that had previously slowed health system investment in integrated virtual health applications.
“We have to operate a hospital within a hospital, taking care of the needs for patients who have had strokes or a newborn delivery or need surgery while dealing with an otherwise healthy 35-year-old who picked up Covid-19 at a social event,” says James Linder, chief executive of Nebraska Medicine…
For instance, more hospitals are remotely triaging and registering patients before they even arrive. Clinicians can consult with patients from their home via telemedicine to help determine how sick they are and if they need to come to the ER at all. From there, admissions are made with as little contact with staff or other patients as possible.
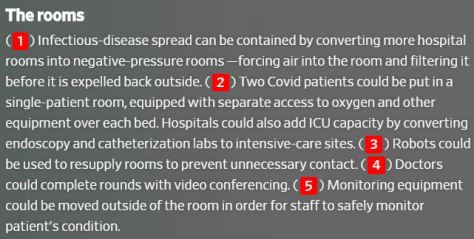
Hospitals are rethinking how they operate in light of the Covid-19 pandemic—and preparing for a future where such crises may become a grim fact of life.
Illustration by Justin Metz
With the potential for resurgences of the coronavirus, and some scientists warning about outbreaks of other infectious diseases, hospitals don’t want to be caught flat-footed again. So, more of them are turning to new protocols and new technology to overhaul standard operating procedure, from the time patients show up at an emergency room through admission, treatment and discharge.
Facing shortages of critical equipment, medical workers must make life-or-death decisions about who receives care. WSJ’s Joe Palazzolo reports from an emergency room that’s running short on ventilators, and Chris Weaver explains the plans hospitals are putting in place to decide who gets them.
Arthur Caplan, a bioethicist at NYU’s School of Medicine, talks about how hospitals think about these difficult choices.
From a Becker’s Hospital Review release (02/19/2020):
Amazon’s virtual medical clinic that offers in-person follow-ups is now available to Amazon employees in Seattle.
Five things to know:
1. The virtual medical service, called Amazon Care, went live via the company’s employee benefits portal on Feb. 18. It is available to Amazon employees who work at the company’s headquarters and their dependents.
2. Amazon Care offers employees virtual medical consultations with physicians and nurse practitioners. Patients can use the app to schedule a follow-up visit in their home or office.
3. Medications prescribed via Amazon Care can be delivered to a patient’s home.
4. “Amazon Care eliminates travel and wait time, connecting employees and their family members to a physician or nurse practitioner through live chat or video, with the option for in-person follow up services from a registered nurse ranging from immunizations to instant strep throat detection,” an Amazon spokesperson told CNBC.
5. Amazon first shared information about Amazon Care in September, noting that it planned to pilot the service in Seattle.
We’ve come a long way since the first heartbeat was heard. This American Heart Month, we take a look at the history of cardiac care — and celebrate the leading-edge innovations that make a better future possible.
This week on Prognosis, we look at one startup that’s trying to redesign care for some of the most vulnerable patients, taking into account the complex realities of their lives. The company is trying to improve care for people and communities the medical system often fails – and it believes that fixing those failures will not only make people healthier, it will also save money.
In America, poverty is linked to shorter lifespans. The wealthiest 1% of Americans live more than a decade longer than the poorest 1%, and the longevity gap has expanded in recent years. The medical community is increasingly examining the role that poverty and difficult social circumstances play in illness. Some people are asking whether the health care system could do more to address the things that influence people’s health beyond their medical care.
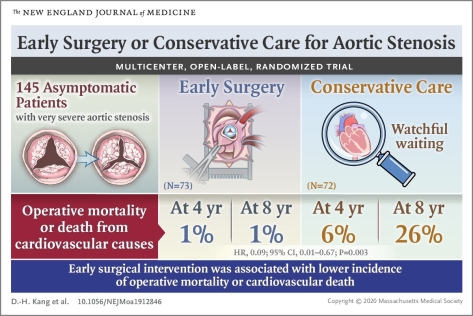
Among asymptomatic patients with very severe aortic stenosis, the incidence of the composite of operative mortality or death from cardiovascular causes during the follow-up period was significantly lower among those who underwent early aortic-valve replacement surgery than among those who received conservative care.
The specialty of emergency medicine is firmly grounded in social justice and providing access to expert care to everyone who comes in. That means treating anyone, with any condition, at any time. And yet, embedded into emergency department operations is a system that might be perceived as unjust: the concept of triage. The emergency queue isn’t “first come, first served.” It’s nonlinear by design, since triage prioritizes the severity of illness. The severely ill or injured receive immediate attention. Everyone else, to various degrees, must wait.
There are situations when waiting feels immoral to me, not merely inconvenient. Being an emergency doctor means shouldering burdens for perceived injustices that we have little, if any, control over. Most of the beds were locked up with patients boarding in the ED, which means they are waiting for an inpatient bed to become available in the hospital.
Hospitals have high expectations regarding how quickly patients are seen in the emergency department, and my colleagues and I share that goal. But there’s less urgency when it comes to discharging patients from the hospital, which would unclog the backup in the emergency department — and its waiting room.





 For instance, more hospitals are remotely triaging and registering patients before they even arrive. Clinicians can consult with patients from their home via telemedicine to help determine how sick they are and if they need to come to the ER at all. From there, admissions are made with as little contact with staff or other patients as possible.
For instance, more hospitals are remotely triaging and registering patients before they even arrive. Clinicians can consult with patients from their home via telemedicine to help determine how sick they are and if they need to come to the ER at all. From there, admissions are made with as little contact with staff or other patients as possible.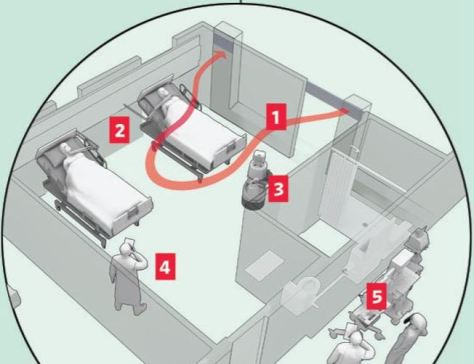
 With the potential for resurgences of the coronavirus, and some scientists warning about outbreaks of other infectious diseases, hospitals don’t want to be caught flat-footed again. So, more of them are turning to new protocols and new technology to overhaul standard operating procedure, from the time patients show up at an emergency room through admission, treatment and discharge.
With the potential for resurgences of the coronavirus, and some scientists warning about outbreaks of other infectious diseases, hospitals don’t want to be caught flat-footed again. So, more of them are turning to new protocols and new technology to overhaul standard operating procedure, from the time patients show up at an emergency room through admission, treatment and discharge.





 Facing shortages of critical equipment, medical workers must make life-or-death decisions about who receives care. WSJ’s Joe Palazzolo reports from an emergency room that’s running short on ventilators, and Chris Weaver explains the plans hospitals are putting in place to decide who gets them.
Facing shortages of critical equipment, medical workers must make life-or-death decisions about who receives care. WSJ’s Joe Palazzolo reports from an emergency room that’s running short on ventilators, and Chris Weaver explains the plans hospitals are putting in place to decide who gets them. 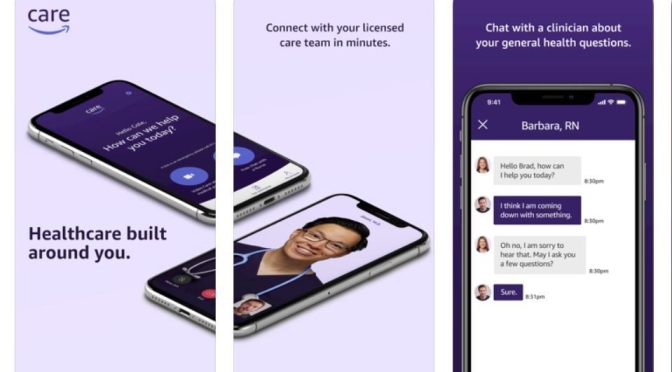
 Amazon’s virtual medical clinic that offers in-person follow-ups is now available to Amazon employees in Seattle.
Amazon’s virtual medical clinic that offers in-person follow-ups is now available to Amazon employees in Seattle. 3. Medications prescribed via Amazon Care can be delivered to a patient’s home.
3. Medications prescribed via Amazon Care can be delivered to a patient’s home.

 This week on Prognosis, we look at one startup that’s trying to redesign care for some of the most vulnerable patients, taking into account the complex realities of their lives. The company is trying to improve care for people and communities the medical system often fails – and it believes that fixing those failures will not only make people healthier, it will also save money.
This week on Prognosis, we look at one startup that’s trying to redesign care for some of the most vulnerable patients, taking into account the complex realities of their lives. The company is trying to improve care for people and communities the medical system often fails – and it believes that fixing those failures will not only make people healthier, it will also save money.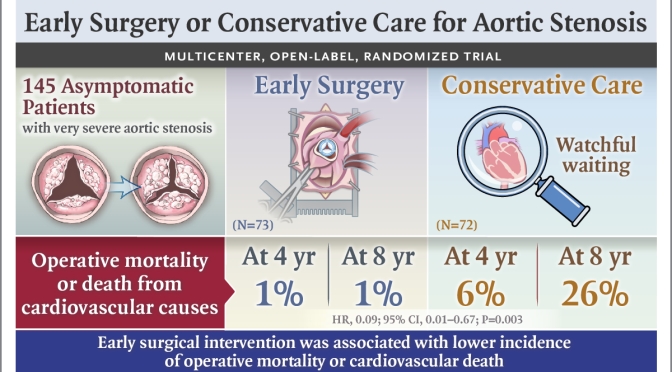

 The
The 