On the Mayo Clinic Radio program, Dr. Jonathan D’Cunha, a Mayo Clinic thoracic surgeon, explains when thoracic surgery might be needed.

On the Mayo Clinic Radio program, Dr. Jonathan D’Cunha, a Mayo Clinic thoracic surgeon, explains when thoracic surgery might be needed.
When is elbow pain an emergency? Can the elbow joint be replaced? What’s that weird feeling when you hit your funny bone? Orthopedic Surgeon, William Seitz Jr., MD, sits down to answer these questions and more.
From a JAMA Network online study (February 11, 2020):
 In this analysis of commercially insured patients who had undergone elective surgery with an in-network surgeon at an in-network facility, approximately 1 in 5 received an out-of-network bill, with a mean potential balance bill of $2011.
In this analysis of commercially insured patients who had undergone elective surgery with an in-network surgeon at an in-network facility, approximately 1 in 5 received an out-of-network bill, with a mean potential balance bill of $2011.
In this retrospective analysis of 347 356 surgical episodes among commercially insured patients who had undergone elective surgery with in-network primary surgeons and facilities, 20% of episodes involved out-of-network charges.
The patterns of out-of-network bills varied with the clinical scenario. Simpler ambulatory procedures that tend to involve 1 surgeon (arthroscopic meniscal repair, breast lumpectomy) had fewer out-of-network bills (13%-15% of cases), whereas inpatient procedures (hysterectomy, knee replacement, colectomy, CABG surgery) had more frequent out-of-network bills (24%-33% of cases). These more complex procedures were also associated with larger potential balance bills, in the range of $2000 to $4000.
Tough to beat! Head #InsideTheOR with S. Christopher Malaisrie, MD, and witness open heart surgery by one of the best cardiology and heart surgery programs in the nation as ranked by US News and World Report.
Doing good is increasingly about more than giving away money. Living kidney donations are rising and a new movement is pushing altruistically minded people to choose careers in fields, such as AI, that will shape the world’s future.
From a News-Medical.net online release:
![]() “Patients can go home after a shorter length of stay in the hospital without increased risk of complications and rehospitalizations,” said Dr. Malaisrie. “Because we found no detrimental effect of accelerated discharge, both patients and physicians should not be averse to discharging patients when medically ready.”
“Patients can go home after a shorter length of stay in the hospital without increased risk of complications and rehospitalizations,” said Dr. Malaisrie. “Because we found no detrimental effect of accelerated discharge, both patients and physicians should not be averse to discharging patients when medically ready.”
Dr. Malaisrie anticipates that the Northwestern Medicine cardiac ERAS program will result in faster recoveries, reduced complications, decreased time in the hospital, lower costs, and improved patient/family satisfaction. In the future, the researchers plan to closely examine both traditional clinical endpoints and patient-reported outcomes from the program.
“Expectations for recovery after cardiac surgery are being reset in the current era,” he said. “What does this mean for patients? It means that prolonged or taxing recovery is no longer required. Patients should know that recovery from heart surgery is not only quicker, but also better with ERAS programs.”
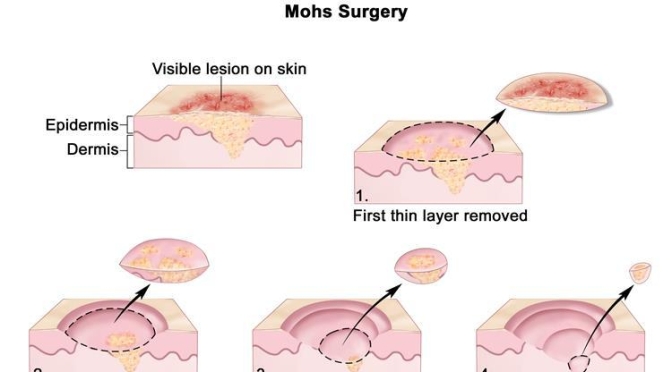
Named after the late Frederic Mohs, M.D., Mohs micrographic surgery is a highly precise excision technique in which the cancer is removed in stages, one tissue layer at a time. After each removal step, the layer is examined under a microscope to determine whether cancer remains in the patient’s skin and, if present, where exactly it is located so that the surgeon can pinpoint where to remove the remaining skin cancer. This allows for the smallest scar and best cosmetic result.
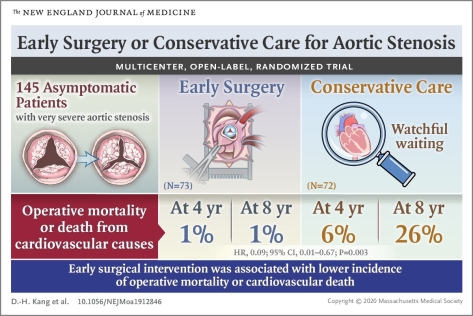
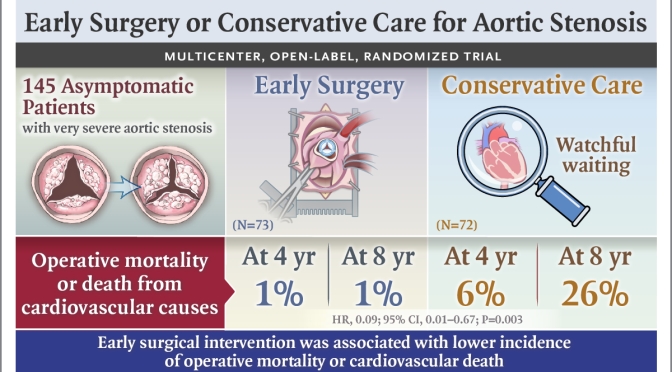
Among asymptomatic patients with very severe aortic stenosis, the incidence of the composite of operative mortality or death from cardiovascular causes during the follow-up period was significantly lower among those who underwent early aortic-valve replacement surgery than among those who received conservative care.
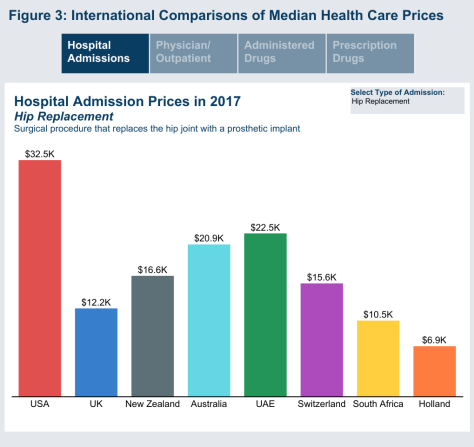
From a Health Care Cost Institute (HCCI) release (12/17/19):