When you’re ready to start reviewing plans, check out the Medicare plan finder tool, which will let you compare Medicare Advantage and Part D prescription drug plans available in your area. You can also get this information by calling Medicare at 800-633-4227.
If you’re looking for a Medigap plan, you can also start at medicare.gov, where you can compare the different types of coverage, as well as find the policies available in your ZIP code.
Another good resource is the State Health Insurance Assistance Program (SHIP), which provides free guidance over the phone. To find your state’s program, go to shiphelp.org or call 877-839-2675.
President Biden has released a health care plan that proposes reducing the age of eligibility for Medicare to 60 years and introducing a public option. Larry Levitt, MPP, Executive Vice President for Health Policy at the Kaiser Family Foundation, and Karen Joynt Maddox, MD, MPH, Co-Director of the Center for Health Economics and Policy (CHEP) at @Washington University School of Medicine, and Lawrence O. Gostin, JD from the O’Neill Institute for National and Global Health Law at Georgetown University discuss prospects for health care reform under the new administration.
If you’re enrolled only in original Medicare with a Medigap supplemental plan, and don’t use a drug plan, there’s no need to re-evaluate your coverage, experts say. But Part D drug plans should be reviewed annually. The same applies to Advantage plans, which often wrap in prescription coverage and can make changes to their rosters of in-network health care providers.
“The amount of information that consumers need to grasp is dizzying, and it turns them off from doing a search,” Mr. Riccardi said. “They feel paralyzed about making a choice, and some just don’t think there is a more affordable plan out there for them.”
Is there another way?
November 13, 2020
When creation of the prescription drug benefit was being debated, progressive Medicare advocates fought to expand the existing program to include drug coverage, funded by a standard premium, similar to the structure of Part B. The standard Part B premium this year is $144.60; the only exceptions to that are high-income enrollees, who pay special income-related surcharges, and very low-income enrollees, who are eligible for special subsidies to help them meet Medicare costs.
“Given the enormous Medicare population that could be negotiated for, I think most drugs could be offered through a standard Medicare plan,” said Judith A. Stein, executive director of the Center for Medicare Advocacy.
“Instead, we have this very fragmented system that assumes very savvy, active consumers will somehow shop among dozens of plan options to see what drugs are available and at what cost with all the myriad co-pays and cost-sharing options,” she added.
Advocates like Ms. Stein also urged controlling program costs by allowing Medicare to negotiate drug prices with pharmaceutical companies — something the legislation that created Part D forbids.
There may be few issues that unite Americans ahead of the 2020 election as do their concerns about the cost of prescription drugs.
A clear majority — 75% — of respondents to a July survey said the cost of prescription medicines would be among the factors likely to influence their votes this year, according to a report from Gallup and the nonprofit West Health. Gallup reported on results from 1,007 interviews conducted with adults between July 1 and July 24.
1. What are the 2020 presidential candidates saying they will do to lower drug prices?
Both President Donald Trump, a Republican, and former Vice President Joe Biden, a Democrat, have highlighted insulin costs in their discussions of the need to lower drug prices.
In a January interview with the New York Times editorial board, Biden noted the widespread discontent among Americans about sticker shock often experienced at pharmacies. He spoke of a need for the federal government to act to make medicines more affordable.
“This is a place where I find, whether you’re Republican or Democrat, you think you’re getting screwed on drug prices. And you are, in terms of everything from insulin to inhalers and a whole range of other things,” Biden said. “So, again, can I guarantee that it gets done? No, but I can tell you what, if anybody can get it done, I can, and I think there’s a consensus for it.”
2. Why doesn’t Medicare, the biggest U.S. purchaser of drugs, directly negotiate on drug prices?
Congress has taken different approaches in designing the terms under which the two largest federal health programs, Medicaid and Medicare, buy drugs.
Medicaid is a program run by states with federal contributions and oversight. It covers people with low incomes and disabilities. Almost 67 million people were enrolled in Medicaid as of May 2020, including about 29 million children. In 1990 Congress decided that drugmakers who want to have their products covered by Medicaid must give rebates to the government. The initial rebate is equal to 23.1% of the average manufacturer price (AMP) for most drugs, or the AMP minus the best price provided to most other private-sector payers, whichever is greater. An additional rebate kicks in when prices rise faster than general inflation.
3. What’s the deal with rebates and discounts?
There’s widespread frustration among lawmakers and policy analysts about the lack of clarity about the role of middlemen in the supply chain for medicines. Known as pharmacy benefit managers (PBMs), these businesses describe the aim of their business as making drugs more affordable for consumers. Insurers like Cigna and UnitedHealth operate some of the nation’s largest PBMs, as does pharmacy giant CVS Health, which also owns insurer Aetna.
“They will tell you their mission is to lower drug costs,” said Rep. Earl L. “Buddy” Carter, a Georgia Republican, a pharmacist and a critic of PBMs, in a speech on the House floor last year. “My question to you would be: How is that working out?”
4. What is the “distinctly American” phenomenon of specialty drugs?
Kesselheim also has written on what he terms “Specialty Drugs — A Distinctly American Phenomenon.” That’s the title of a 2020 paper in the New England Journal of Medicine Kesselheim authored with Huseyin Naci, an associate professor of health policy at the London School of Economics.
In this Perspective article, Kesselheim and Naci look at how the “specialty” designation morphed from its origin in the 1970s. It then referred to a need for extra steps for preparation and delivery of new injectable and infusion products.
5. How much does it cost to bring a new drug to market anyway?
The median cost for a medicine developed in recent years was $985 million, according to a study published in JAMA in March 2020, “Estimated Research and Development Investment Needed to Bring a New Medicine to Market, 2009-2018.”
“Rising drug prices have attracted public debate in the United States and abroad on fairness of drug pricing and revenues,” write the study’s authors: Olivier J. Wouters of the London School of Economics; Martin McKee of the London School of Hygiene and Tropical Medicine; and Jeroen Luyten of Leuven Institute for Healthcare Policy, KU Leuven, Belgium. “Central to this debate is the scale of research and development investment by companies that is required to bring new medicines to market.”
As we head into South Carolina’s primary and gear up for Super Tuesday, the 2020 candidates are looking to stand out to voters. But perhaps no policy proposal has marked this election more than Sen. Bernie Sanders’s push for Medicare for All.
While the Democratic candidates agree on expanding health coverage, they’re divided on how to insure everyone, whether to insure everyone, and, of course, how to pay for it all.
So how are they similar? How are they different? And how does that compare to President Trump?
Rachana Pradhan, correspondent for Kaiser Health News; Noam Levey, national healthcare reporter for The LA Times; and Dan Diamond, health reporter for Politico and host of the “Pulse Check” podcast helped us break down where each candidate stood on health care.
From a Wall Street Journal Opinion article (Feb 10, 2020):
How to address the elder-care crisis? Ideally, doctors would screen older patients for dementia. An early diagnosis helps patients understand treatment options, plan for the future and receive appropriate care in the hospital.
Other steps include: more preventive care, changes to Medicare’s rehabilitation policies, adopting new reimbursement methods, and developing new measures of success. Primary-care offices can prevent hospital visits, but Americans seeking primary care face an average wait time of 24 days. This might not be a problem for a patient in need of an annual physical, but conditions like chest pain or infections require prompt treatment. Primary-care offices that offer same-day sick visits, home visits for bed-bound older adults, or at-home monitoring of conditions could reduce emergency department volumes.
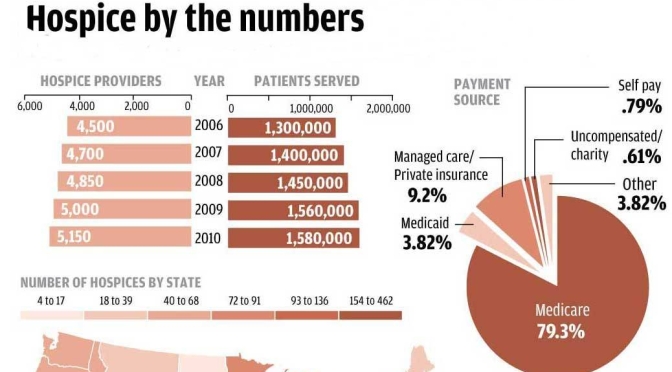
According to a recent Kaiser Family Foundation poll, seven in 10 Americans say they would prefer to die at home. And that’s the direction the health care system is moving, too, hoping to avoid unnecessary and expensive treatment at the end of life.
Hospice allows a patient deemed to have fewer than six months to live to change the focus of their medical care — from the goal of curing disease to a new goal of using treatments and medicines to maintain comfort and quality of life. It is a form of palliative care, which also focuses on pain management, but can be provided while a patient continues to seek a cure or receive treatments to prolong life.
Seema Verma, administrator for the Centers for Medicare and Medicaid Services, sits down for a rare one-on-one interview with special correspondent Sarah Varney of Kaiser Health News. They discuss President Trump’s plan for sustaining public health insurance programs, how the administration would respond if Obamacare is struck down by the courts in the future, and the latest Medicare for all proposals.
Medicare negotiation of prescription-drug prices would bring U.S. government policies in line with those of other high-income countries, and the idea is popular with both the public and policy analysts. But it would represent a sea change for pharmaceutical firms, which will maintain that any threat to their pricing power will slow innovation.
Negotiating prices of 10 too-little drugs and 10 too-late drugs to levels currently paid in the United Kingdom would produce about $26.8 billion in savings in 2019 alone, most of which ($25.9 billion) would come from savings on drugs in the latter category. Over time, the drugs included could change. For instance, in 2020 this category might include Revlimid (lenalidomide), which generated $6.5 billion in 2018 U.S. sales; its price in the United Kingdom is 32% of that in the United States.
Americans all along the political spectrum favor allowing Medicare to negotiate the prices it pays for prescription drugs.1 In September, House Speaker Nancy Pelosi (D-CA) introduced what is now called the Elijah E. Cummings Lower Drug Costs Now Act of 2019 (H.R. 3), and the bill would have Medicare do just that.
Although there are draft pieces of legislation and regulation that take aim at the rising cost of drugs, H.R. 3 is the legislative tip of the spear for price negotiation. If it became law, Medicare would target drugs that claim the largest share of the health care budget and that face limited competition from generics or biosimilars. I propose an alternative set of drugs for price negotiation: those that have too little evidence to support full approval or are too late in their life cycle to justify continued high prices.













 As we head into South Carolina’s primary and gear up for Super Tuesday, the 2020 candidates are looking to stand out to voters. But perhaps no policy proposal has marked this election more than Sen. Bernie Sanders’s push for Medicare for All.
As we head into South Carolina’s primary and gear up for Super Tuesday, the 2020 candidates are looking to stand out to voters. But perhaps no policy proposal has marked this election more than Sen. Bernie Sanders’s push for Medicare for All.


 Medicare negotiation of prescription-drug prices would bring U.S. government policies in line with those of other high-income countries, and the idea is popular with both the public and policy analysts. But it would represent a sea change for pharmaceutical firms, which will maintain that any threat to their pricing power will slow innovation.
Medicare negotiation of prescription-drug prices would bring U.S. government policies in line with those of other high-income countries, and the idea is popular with both the public and policy analysts. But it would represent a sea change for pharmaceutical firms, which will maintain that any threat to their pricing power will slow innovation. 