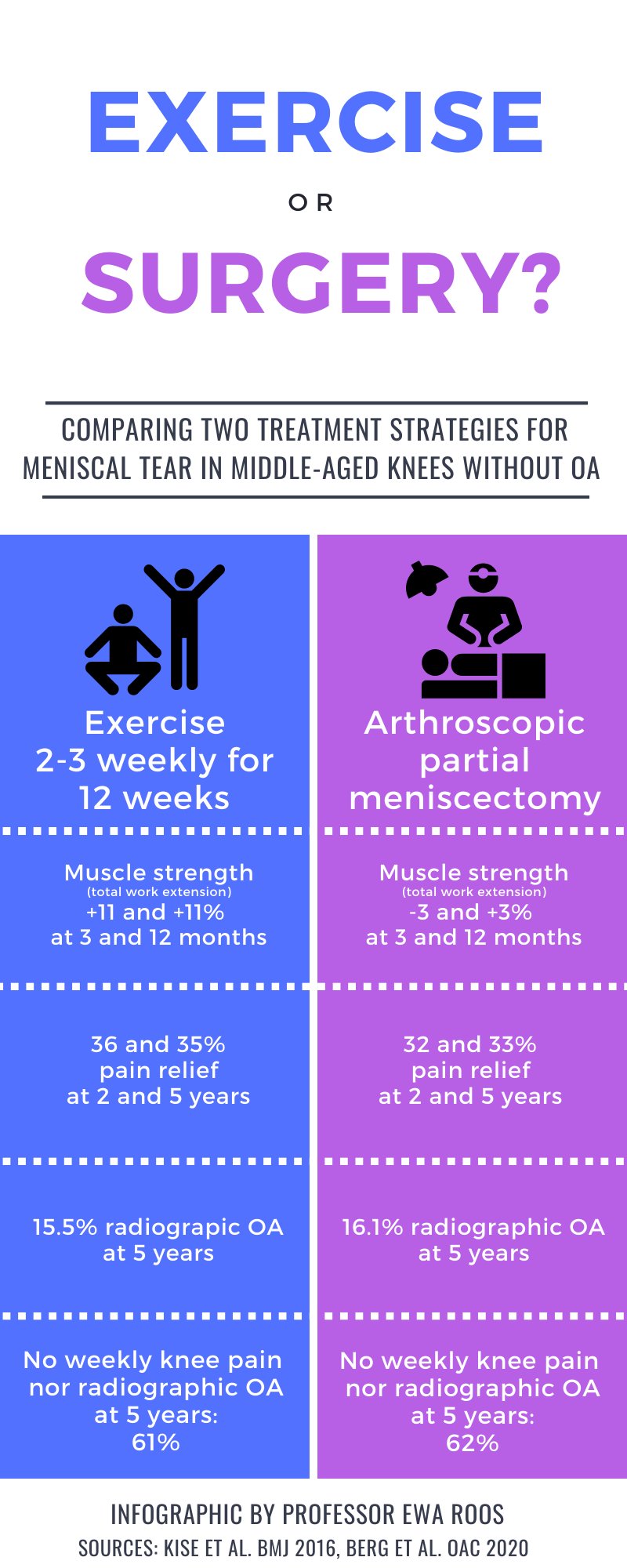
Conclusion: The study was inconclusive with respect to potential differences in progression of individual radiographic features after surgical and non-surgical treatment for degenerative meniscal tear. Further, we found no strong evidence in support of differences in development of incident radiographic knee osteoarthritis or patient-reported outcomes between exercise therapy and arthroscopic partial meniscectomy.
Objective: To evaluate progression of individual radiographic features 5 years following exercise therapy or arthroscopic partial meniscectomy as treatment for degenerative meniscal tear.
Design: Randomized controlled trial including 140 adults, aged 35-60 years, with a magnetic resonance image verified degenerative meniscal tear, and 96% without definite radiographic knee osteoarthritis. Participants were randomized to either 12-weeks of supervised exercise therapy or arthroscopic partial meniscectomy. The primary outcome was between-group difference in progression of tibiofemoral joint space narrowing and marginal osteophytes at 5 years, assessed semi-quantitatively by the OARSI atlas. Secondary outcomes included incidence of radiographic knee osteoarthritis and symptomatic knee osteoarthritis, medial tibiofemoral fixed joint space width (quantitatively assessed), and patient-reported outcome measures. Statistical analyses were performed using a full analysis set. Per protocol and as treated analysis were also performed.
Results: The risk ratios (95% CI) for progression of semi-quantitatively assessed joint space narrowing and medial and lateral osteophytes for the surgery group were 0.89 (0.55-1.44), 1.15 (0.79-1.68) and 0.77 (0.42-1.42), respectively, compared to the exercise therapy group. In secondary outcomes (full-set analysis) no statistically significant between-group differences were found.
Read full study




 In studies of aerobic exercise in patients with knee OA, very few interventions met guideline-recommended dose; there were small to moderate changes in markers of cardiovascular health and no decrease in markers of systemic inflammation. These findings question whether aerobic exercise is being used to its full potential in patients with knee OA.
In studies of aerobic exercise in patients with knee OA, very few interventions met guideline-recommended dose; there were small to moderate changes in markers of cardiovascular health and no decrease in markers of systemic inflammation. These findings question whether aerobic exercise is being used to its full potential in patients with knee OA.
 Researchers matched 7,743 people with osteoarthritis with 23,229 healthy people who rarely or never took NSAIDs. People with osteoarthritis had a 42% higher risk of heart failure and a 17% higher risk of coronary artery disease compared with healthy people. After controlling for a range of factors that contribute to heart disease (including high body mass index, high blood pressure, and diabetes), they concluded that 41% of the increased risk of heart disease related to osteoarthritis was due to the use of NSAIDs.
Researchers matched 7,743 people with osteoarthritis with 23,229 healthy people who rarely or never took NSAIDs. People with osteoarthritis had a 42% higher risk of heart failure and a 17% higher risk of coronary artery disease compared with healthy people. After controlling for a range of factors that contribute to heart disease (including high body mass index, high blood pressure, and diabetes), they concluded that 41% of the increased risk of heart disease related to osteoarthritis was due to the use of NSAIDs.