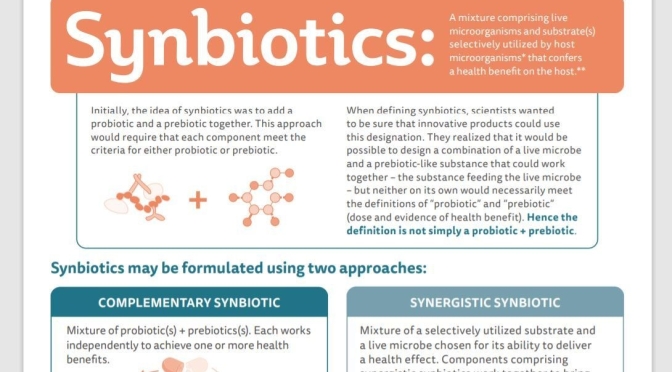

New Health Infographics: “What Are Synbiotics?”


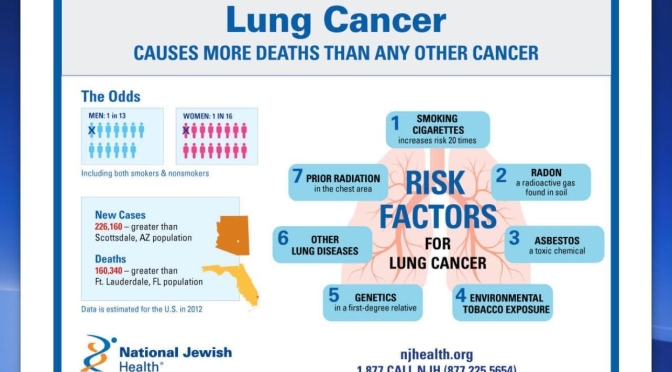
NEJM (Aug 13, 2020) – Population-level mortality from NSCLC in the United States fell sharply from 2013 to 2016, and survival after diagnosis improved substantially. Our analysis suggests that a reduction in incidence along with treatment advances — particularly approvals for and use of targeted therapies — is likely to explain the reduction in mortality observed during this period.
“The survival benefit for patients with non-small cell lung cancer treated with targeted therapies has been demonstrated in clinical trials, but this study highlights the impact of these treatments at the population level,” said Nadia Howlader, Ph.D., of NCI’s Division of Cancer Control and Population Sciences, who led the study. “We can now see the impact of advances in lung cancer treatment on survival.”




There is consistent evidence that moderate reductions (i.e. a decrease of 3 to 5 g or ½ to 1 teaspoon a day) in salt intake can lead to a reduction in blood pressure.5,6 However, these effects may not be the same for everyone and will depend on an individual’s starting blood pressure (greater benefits are seen in those with higher blood pressure), their current level of salt intake, genetics, disease status and medication use.
It is important to note that salt is not the only lifestyle factor that can influence our blood pressure. Other factors such as eating enough potassium, maintaining a healthy body weight, not smoking, and being physically active are also important when it comes to reducing blood pressure. You can find 7 lifestyle tips to help reduce blood pressure here.

Salt is the common name for sodium chloride (or NaCl). It consists of 40% sodium and 60% chloride. In other words, 2.5 g of salt contains 1 g of sodium and 1.5 g of chloride.
Both sodium and chloride are essential for many body functions. They help regulate blood pressure, control fluid balance, maintain the right conditions for muscle and nerve function and allow for the absorption and transport of nutrients across cell membranes. Chloride is also used to produce stomach acid (hydrochloric acid, HCl) which helps us digest foods.
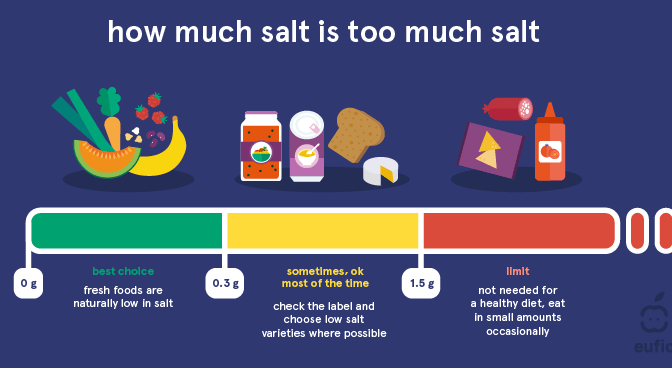
The exact minimum daily requirement for salt is unknown, but it is thought to be around 1.25 g – 2.5 g (0.5 – 1 g sodium) per day.1 As salt is found in a large variety of foods the risk of deficiency is low.1,2 The European Food Safety Authority (EFSA) has stated that a salt intake of 5 g per day (equivalent to 2 g of sodium) is sufficient to meet both our sodium and chloride requirements as well as reduce our risk of high blood pressure and heart disease.1,2 This is equivalent to around 1 teaspoon of salt per day from all sources.
Both sodium and chloride are released from our body through our urine and when we sweat. This means bouts of heavy sweating such as during exercise can increase our salt requirements slightly. However, as most people consume well above required levels it is usually not necessary to increase salt intake during these conditions.1
![]()

“We are learning that tactics to avoid dementia begin early and continue throughout life, so it’s never too early or too late to take action,” says commission member and AAIC presenter Lon Schneider, MD, co-director of the USC Alzheimer Disease Research Center‘s clinical core and professor of psychiatry and the behavioral sciences and neurology at the Keck School of Medicine of USC.
LOS ANGELES — Modifying 12 risk factors over a lifetime could delay or prevent 40% of dementia cases, according to an updated report by the Lancet Commission on dementia prevention, intervention and care presented at the Alzheimer’s Association International Conference (AAIC 2020).
Twenty-eight world-leading dementia experts added three new risk factors in the new report — excessive alcohol intake and head injury in mid-life and air pollution in later life. These are in addition to nine factors previously identified by the commission in 2017: less education early in life; mid-life hearing loss, hypertension and obesity; and smoking, depression, social isolation, physical inactivity and diabetes later in life (65 and up).
Schneider and commission members recommend that policymakers and individuals adopt the following interventions: