

From a Scientific American online article:
 Health care is a big business, and our system reimburses hospitals and health care workers for caring for the sickest people rather than healthiest ones. This process depletes healers’ energy and often causes them to become exhausted and sick. That means all of us who work in or study to work in health care are at risk. To break this vicious cycle, we need self-scrutiny and willingness to change.
Health care is a big business, and our system reimburses hospitals and health care workers for caring for the sickest people rather than healthiest ones. This process depletes healers’ energy and often causes them to become exhausted and sick. That means all of us who work in or study to work in health care are at risk. To break this vicious cycle, we need self-scrutiny and willingness to change.
Health-professions students and workers live in chronically stressful environments—responsible for an increasingly sick population, which they are expected to repeatedly rescue from failure. To heal others, our health care professionals need healing themselves.
American medical students, physicians and nurses: There’s good news and bad news.
The bad news is that our health care system and many of its workers are sick. The good news is that we can heal them. We should waste no time in starting.
To read more: https://blogs.scientificamerican.com/observations/american-health-care-is-sick-and-its-workers-are-too/

 “What is memory without forgetting?” asks Oliver Hardt, a cognitive psychologist studying the neurobiology of memory at McGill University in Montreal, Canada. “It’s impossible,” he says. “To have proper memory function, you have to have forgetting.”
“What is memory without forgetting?” asks Oliver Hardt, a cognitive psychologist studying the neurobiology of memory at McGill University in Montreal, Canada. “It’s impossible,” he says. “To have proper memory function, you have to have forgetting.”
 Now, researchers have developed a fast-acting skin patch that efficiently delivers medication to attack melanoma cells. The device, tested in mice and human skin samples, is an advance toward developing a vaccine to treat melanoma and has widespread applications for other vaccines.
Now, researchers have developed a fast-acting skin patch that efficiently delivers medication to attack melanoma cells. The device, tested in mice and human skin samples, is an advance toward developing a vaccine to treat melanoma and has widespread applications for other vaccines.
 In sarcoidosis, abnormal collections of cells called granulomas invade the organ, interfering with its normal activity and often destroying the surrounding tissue. What is left is a scar, known as fibrosis, dotted with these abnormal granulomas.
In sarcoidosis, abnormal collections of cells called granulomas invade the organ, interfering with its normal activity and often destroying the surrounding tissue. What is left is a scar, known as fibrosis, dotted with these abnormal granulomas.
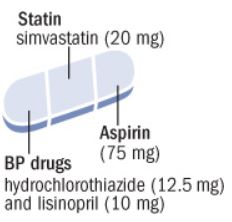 Use of polypill was effective in preventing major cardiovascular events. Medication adherence was high and adverse event numbers were low. The polypill strategy could be considered as an additional effective component in controlling cardiovascular diseases, especially in LMICs.
Use of polypill was effective in preventing major cardiovascular events. Medication adherence was high and adverse event numbers were low. The polypill strategy could be considered as an additional effective component in controlling cardiovascular diseases, especially in LMICs.
 The use of n-3 FA (4 g/d) for improving atherosclerotic cardiovascular disease risk in patients with hypertriglyceridemia is supported by a 25% reduction in major adverse cardiovascular events in REDUCE-IT (Reduction of Cardiovascular Events With EPA Intervention Trial), a randomized placebo-controlled trial of EPA-only in high-risk patients treated with a statin.
The use of n-3 FA (4 g/d) for improving atherosclerotic cardiovascular disease risk in patients with hypertriglyceridemia is supported by a 25% reduction in major adverse cardiovascular events in REDUCE-IT (Reduction of Cardiovascular Events With EPA Intervention Trial), a randomized placebo-controlled trial of EPA-only in high-risk patients treated with a statin.
 This joint position statement from the International Atherosclerosis Society and the International Chair on Cardiometabolic Risk Working Group on Visceral Obesity summarises the evidence for visceral adiposity and ectopic fat as emerging risk factors for type 2 diabetes, atherosclerosis, and cardiovascular disease, with a focus on practical recommendations for health professionals and future directions for research and clinical practice.
This joint position statement from the International Atherosclerosis Society and the International Chair on Cardiometabolic Risk Working Group on Visceral Obesity summarises the evidence for visceral adiposity and ectopic fat as emerging risk factors for type 2 diabetes, atherosclerosis, and cardiovascular disease, with a focus on practical recommendations for health professionals and future directions for research and clinical practice.



 For the study, nearly 8,300 people at risk for heart disease had fasting and nonfasting lipid profile tests done at least four weeks apart. (Fasting means they had nothing to eat or drink except water for at least eight hours before the test.) The differences in their total, LDL, and HDL cholesterol values were negligible. Triglyceride levels were modestly higher in the nonfasting samples.
For the study, nearly 8,300 people at risk for heart disease had fasting and nonfasting lipid profile tests done at least four weeks apart. (Fasting means they had nothing to eat or drink except water for at least eight hours before the test.) The differences in their total, LDL, and HDL cholesterol values were negligible. Triglyceride levels were modestly higher in the nonfasting samples.
 Slower speech, for example, could indicate fatigue or sorrow at one point in time, but over longer periods could signal something more severe, co-founder Jim Harper said.
Slower speech, for example, could indicate fatigue or sorrow at one point in time, but over longer periods could signal something more severe, co-founder Jim Harper said.