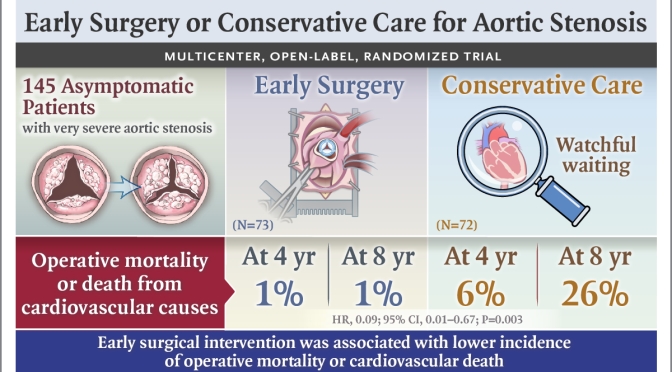
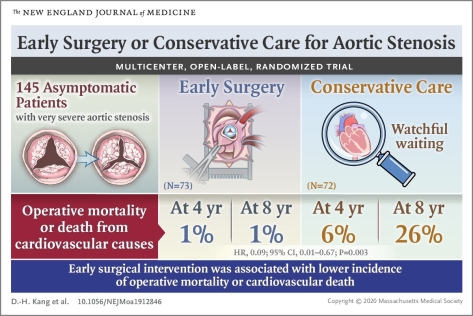
Among asymptomatic patients with very severe aortic stenosis, the incidence of the composite of operative mortality or death from cardiovascular causes during the follow-up period was significantly lower among those who underwent early aortic-valve replacement surgery than among those who received conservative care.
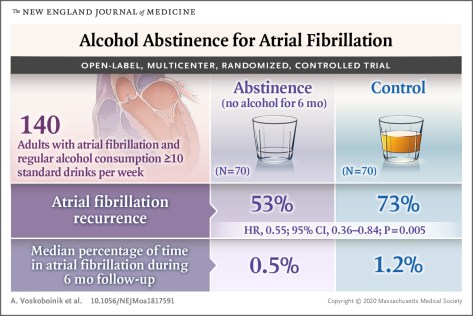
Abstinence from alcohol reduced arrhythmia recurrences in regular drinkers with atrial fibrillation.
January 2, 2020 Atrial fibrillation is the most common sustained arrhythmia,1 and alcohol is consumed by a majority of U.S. adults.2 The current study showed that among regular drinkers, a substantial reduction in alcohol consumption by patients with symptomatic atrial fibrillation was associated with a reduction in recurrence of atrial fibrillation and a reduced proportion of time spent in atrial fibrillation. Earlier meta-analyses showed that alcohol was associated with a dose-related increased risk of incident atrial fibrillation, with increased risk observed even among drinkers who consumed as few as 7 drinks per week.8 Current trends show a rise in alcohol consumption among adults older than 60 years of age,2coupled with greater prevalence of atrial fibrillation in this age group. The present study, with participants having an average intake of approximately 17 drinks per week at baseline, suggests that consumption at these levels may contribute to atrial fibrillation.
Medicare negotiation of prescription-drug prices would bring U.S. government policies in line with those of other high-income countries, and the idea is popular with both the public and policy analysts. But it would represent a sea change for pharmaceutical firms, which will maintain that any threat to their pricing power will slow innovation.
Negotiating prices of 10 too-little drugs and 10 too-late drugs to levels currently paid in the United Kingdom would produce about $26.8 billion in savings in 2019 alone, most of which ($25.9 billion) would come from savings on drugs in the latter category. Over time, the drugs included could change. For instance, in 2020 this category might include Revlimid (lenalidomide), which generated $6.5 billion in 2018 U.S. sales; its price in the United Kingdom is 32% of that in the United States.
Americans all along the political spectrum favor allowing Medicare to negotiate the prices it pays for prescription drugs.1 In September, House Speaker Nancy Pelosi (D-CA) introduced what is now called the Elijah E. Cummings Lower Drug Costs Now Act of 2019 (H.R. 3), and the bill would have Medicare do just that.
Although there are draft pieces of legislation and regulation that take aim at the rising cost of drugs, H.R. 3 is the legislative tip of the spear for price negotiation. If it became law, Medicare would target drugs that claim the largest share of the health care budget and that face limited competition from generics or biosimilars. I propose an alternative set of drugs for price negotiation: those that have too little evidence to support full approval or are too late in their life cycle to justify continued high prices.




 Medicare negotiation of prescription-drug prices would bring U.S. government policies in line with those of other high-income countries, and the idea is popular with both the public and policy analysts. But it would represent a sea change for pharmaceutical firms, which will maintain that any threat to their pricing power will slow innovation.
Medicare negotiation of prescription-drug prices would bring U.S. government policies in line with those of other high-income countries, and the idea is popular with both the public and policy analysts. But it would represent a sea change for pharmaceutical firms, which will maintain that any threat to their pricing power will slow innovation. 