Conclusion: The study was inconclusive with respect to potential differences in progression of individual radiographic features after surgical and non-surgical treatment for degenerative meniscal tear. Further, we found no strong evidence in support of differences in development of incident radiographic knee osteoarthritis or patient-reported outcomes between exercise therapy and arthroscopic partial meniscectomy.
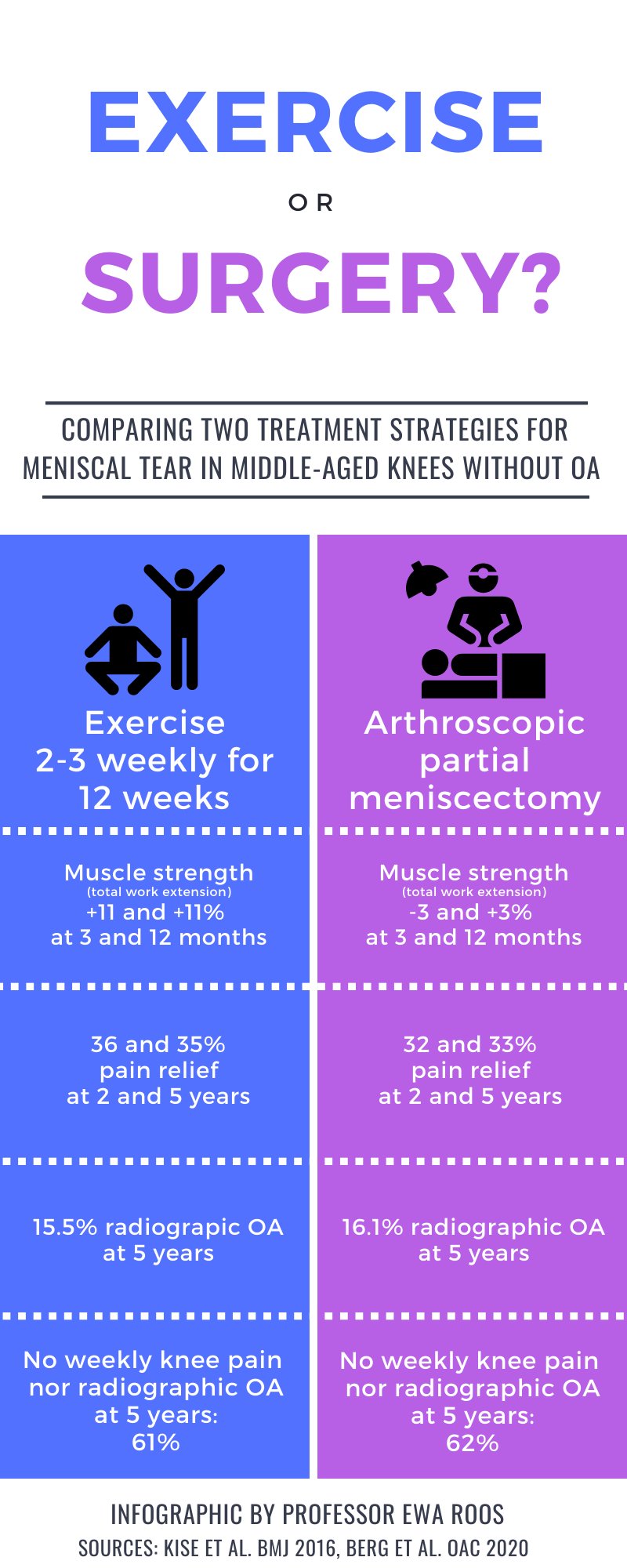
Objective: To evaluate progression of individual radiographic features 5 years following exercise therapy or arthroscopic partial meniscectomy as treatment for degenerative meniscal tear.
Design: Randomized controlled trial including 140 adults, aged 35-60 years, with a magnetic resonance image verified degenerative meniscal tear, and 96% without definite radiographic knee osteoarthritis. Participants were randomized to either 12-weeks of supervised exercise therapy or arthroscopic partial meniscectomy. The primary outcome was between-group difference in progression of tibiofemoral joint space narrowing and marginal osteophytes at 5 years, assessed semi-quantitatively by the OARSI atlas. Secondary outcomes included incidence of radiographic knee osteoarthritis and symptomatic knee osteoarthritis, medial tibiofemoral fixed joint space width (quantitatively assessed), and patient-reported outcome measures. Statistical analyses were performed using a full analysis set. Per protocol and as treated analysis were also performed.
Results: The risk ratios (95% CI) for progression of semi-quantitatively assessed joint space narrowing and medial and lateral osteophytes for the surgery group were 0.89 (0.55-1.44), 1.15 (0.79-1.68) and 0.77 (0.42-1.42), respectively, compared to the exercise therapy group. In secondary outcomes (full-set analysis) no statistically significant between-group differences were found.
Read full study