
There are two types of stroke:
A transient ischemic attack (TIA) is sometimes called a “mini-stroke.” It is different from the major types of stroke, because blood flow to the brain is blocked for only a short time—usually no more than 5 minutes.1
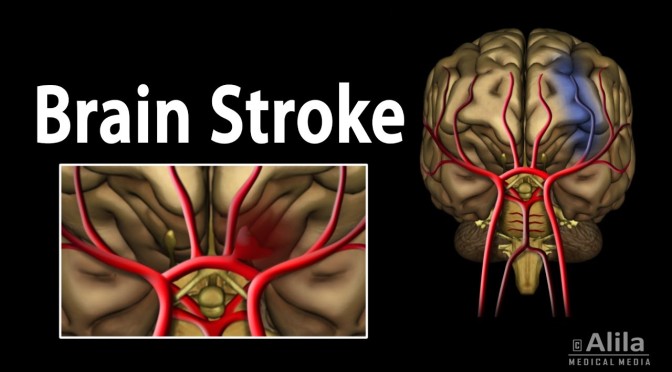
Ischemic stroke
Most strokes are ischemic strokes.2 An ischemic stroke occurs when blood clots or other particles block the blood vessels to the brain.
Fatty deposits called plaque can also cause blockages by building up in the blood vessels.
Hemorrhagic stroke
A hemorrhagic stroke happens when an artery in the brain leaks blood or ruptures (breaks open). The leaked blood puts too much pressure on brain cells, which damages them.
High blood pressure and aneurysms—balloon-like bulges in an artery that can stretch and burst—are examples of conditions that can cause a hemorrhagic stroke.
Transient ischemic attack (TIA or “mini-stroke”)
For Blanche Teal-Cruise, a smoker for 40 years who also had high blood pressure, the transient ischemic attack (sometimes called a mini-stroke) she had on the way to work was a wake-up call. Read Blanche’s story.
TIAs are sometimes known as “warning strokes.” It is important to know that
- A TIA is a warning sign of a future stroke.
- A TIA is a medical emergency, just like a major stroke.
- Strokes and TIAs require emergency care. Call 9-1-1 right away if you feel signs of a stroke or see symptoms in someone around you.
- There is no way to know in the beginning whether symptoms are from a TIA or from a major type of stroke.
- Like ischemic strokes, blood clots often cause TIAs.
- More than a third of people who have a TIA and don’t get treatment have a major stroke within 1 year. As many as 10% to 15% of people will have a major stroke within 3 months of a TIA.1
Recognizing and treating TIAs can lower the risk of a major stroke. If you have a TIA, your health care team can find the cause and take steps to prevent a major stroke.